This classification applies to the entire gastrointestinal tract. In the colon, however, there are additional characteristics which must be taken into account. On the one hand, in contrast to the upper GI tract, a single resection can be regarded as curative, even if the submucosa is infiltrated up to 1,000 μm and a so-called “low-risk” constellation is described (G1/2, L0, V0, R0). Furthermore, it should be noted that pT1 carcinomas in the colorectum always infiltrate the submucosa by definition. For mucosal carcinomas or pTis, the term “high-grade intraepithelial neoplasia / dysplasia” applies here.
It should also be considered that in the colon most lesions are adenomas (mostly tubulo / tubulo-villous with low-grade dysplasia). The size of the lesion plays an essential role in polypoid findings (Ip and Is) (although the Paris classification in the general sense only describes lesions less than 2 cm). Furthermore, in the colon, there is good evidence that not only the general appearance of the lesion, but also the surface structure of the mucosa should be appreciated in order to estimate the malignant potential of a lesion (see also www.endoscopy-campus.com/en/klassifikationen/nice-klassifikationen-zur-colonpolypen-differentialdiagnose/).
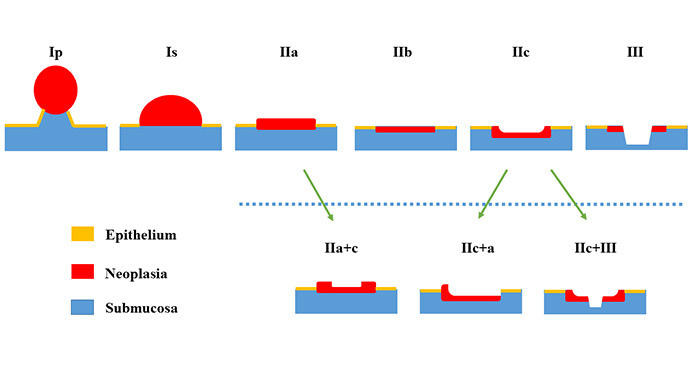
Last but not least, the so-called “lateral spreading tumors” (LST) must be taken into account as an additional subgroup of the type IIa lesions. This subgroup is subdivided again because different characteristics of the LSTs imply a different neoplastic potential and should therefore also be treated differently. LSTs are always larger than 2 cm (!) and are called “LST of granular-type” or “LST of non-granular type”. The group of “LST-granular homogenous” are the most common among these. Despite their sometimes considerable size, they almost always bear a low malignant potential (low grade dysplasia). In the case of the “nodular mixed type”, the size of the node probably plays a role, since in the case of nodular parts greater than 1 cm, a higher degree of neoplasia is frequently present. “Nongranular LSTs” bear a greater malignant potential. In several studies, the rates of submucosal invasive carcinomas in both forms are about 1–3% (granular) versus up to 15% (non-granular). Depressed non-granular lesions appear to bear the highest risk.
Read the Article: https://www.endoscopy-campus.com/en/klassifikationen/paris-classification-of-superficial-tumors-in-the-colon/