I took the long walk today. The long walk from the operating room to the frozen section pathology suite to a consultation room in the surgical waiting area. The family of the patient whose operation I had just completed was waiting expectantly and fearfully in the room. I was out way too soon. I had started the operation less than an hour before.
The patient I operated on has a hilar cholangiocarcinoma, a tumor at the bifurcation of the right and left bile ducts joining into the single proper hepatic duct at the base of the liver. Bile drains out of these bile ducts into the common bile duct running through the pancreas to release bile into the first part of the small intestine, the duodenum. This patient was diagnosed with this tumor at the end of last year when his eyes and skin suddenly and rapidly became bright yellow in color. He saw a primary care physician who ordered an ultrasound which revealed dilated bile ducts throughout the liver. The primary doctor immediately referred him to a gastroenterologist who performed an ERCP (endoscopic retrograde cholangiopancreatography), a procedure where a scope is advanced into the bile duct where it exits into the duodenum. This procedure revealed a tumor blocking the right and left bile ducts at the hilum, or base, of the liver. The gastroenterologist was able to pass a stent tube into the right side bile ducts and a gush of bile from the blocked right-sided biliary tree resulted. He was not able to get a stent into the left-sided bile ducts but he successfully obtained biopsies of the tumor which confirmed the presence of an adenocarcinoma of the bile duct. The patient’s jaundice resolved quickly following the stent placement and he was referred to a medical oncologist.
CT scan showing the dilated bile ducts within the liver caused by a Klatskin tumor.
Chemo-radiation therapy
The medical oncologist completed a thorough staging evaluation including blood tests. One of these blood tests, a CA19-9, was abnormally high. This blood test is elevated in some patients with cancer originating in either the pancreas or the bile duct system, including the gallbladder. A CT scan revealed no evidence of spread of this cancer to the lung or other sites, and demonstrated the presence of a solitary 3 cm tumor obstructing the left sided bile ducts completely with atrophy, or shrinkage, of the left liver, but with decompression of the previously dilated bile ducts of the right liver. There were some enlarged, suspicious lymph nodes around the blood vessels at the base of the liver suggesting the cancer had metastasized to regional lymph nodes. There was no imaging evidence of any distant spread to other organs or sites.
The tumor was clearly invading and damaging the left lobe of the liver, obstructing both the left-sided bile ducts and portal vein, and was creeping far enough up the right side bile ducts that a course of neoadjuvant chemo-radiation therapy was prescribed. The neoadjuvant therapy is delivered preoperatively in an attempt to reduce the size of the tumor and increase the probability of a margin-negative surgical resection. The patient was referred to me before he began his neoadjuvant therapy and I agreed this was a good plan and would improve the chances of complete removal of his malignant bile duct tumor.
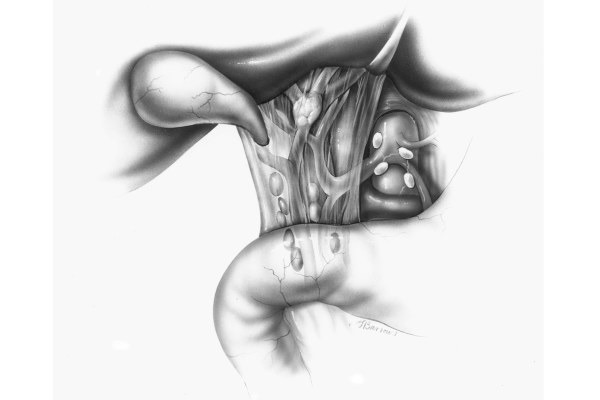
Drawing of the Klatskin tumor in the liver.
The patient completed five weeks of chemo-radiation therapy with minimal problems or side effects. He was active, eating a healthy diet, and walking on a daily basis. I saw him back four weeks after completing the chemo-radiation and a repeat CT scan revealed the tumor had decreased in size by almost 40%, and the lymph nodes near the tumor were also smaller in size. There was still no suggestion of any metastatic disease at any site. I had a long conversation with the patient and his family and we set a surgical date.
Planning the surgery
I met with the patient and his family yesterday in the office and I discussed the proposed operation in detail. As I always do, I used anatomic diagrams and drawings I made while speaking with them to explain what I was planning to do. The goal was to remove the entire damaged left lobe of the liver along with the extrahepatic bile duct system, including a portion of the right bile duct and the gallbladder along with all of the lymph nodes in the area around the base of the liver and between the stomach and the liver. This operation has an impressive, long name: en bloc extended left hepatectomy and resection of the extra hepatic bile duct with porta hepatis lymphadenectomy and Roux Y hepaticojejunostomy. The extended left hepatectomy includes resection of segment 1 of the liver, a caudate lobectomy. This portion of the liver is behind the bile ducts lying atop the inferior vena cava and is frequently invaded by a hilar cholangiocarcinoma, so removal of this liver segment is a critical component of the operation to assure all cancer is removed with negative, or so-called R0, margins. The Roux Y hepaticojejunostomy denotes the portion of the operation where the remaining right bile duct is sewn directly to a loop of small intestine to allow normal drainage of bile into the intestine. I mentioned I anticipated the operation would be completed in approximately five to six hours if all went according to plan.
After describing the operation in detail and reviewing the daunting list of potential intra-operative and post-operative complications, I added a final cautionary note. I informed the patient and his family it was possible, despite the clear CT scans, I could discover spread of disease as noncontiguous liver metastases or peritoneal carcinomatosis, meaning tumor nodules within the belly cavity. No evidence of this type of metastatic spread of disease was demonstrated on any of his imaging studies, but this cancer is nefarious and has a propensity to spread in this fashion in some patients. They voiced their understanding of this possible occurrence but were upbeat and assured me they were confident in the outcome of the operation and in my skill to perform it successfully.
Surgery: Nodules everywhere
Prescience is a worrisome circumstance in oncology. This morning I was fretful for reasons I could not explain. I suppose I can call it a bad feeling. The operation began with a small laparotomy incision from the end of the patient’s breast bone to a point midway between that spot and the belly button. We opened the peritoneal cavity and I swept my hand along the peritoneal surfaces and into the pelvis. My heart sunk and I uttered a curse word. Actually, I muttered a few more under my breath as I palpated more of the lining and organs of the peritoneal cavity. I felt tumor nodules everywhere. The chief resident operating with me repeated my maneuver and shook his head sadly. In a moment we had gone from buoyant and energized to deflated and defeated. We biopsied several of these tumor nodules and sent them for frozen section pathologic analysis to confirm they were metastatic adenocarcinoma. While awaiting the frozen section results, we completed an intra-operative ultrasound of the liver. This confirmed the presence of the tumor mass at the confluence of the bile ducts at the base of the liver with tumor clearly invading the caudate lobe and extending up into the left lobe of the liver. The left lobe was shrunken and damaged from the chronic obstruction of the bile duct. Tumor was also seen creeping up the right-sided bile ducts well into the liver meaning this tumor was not surgically resectable even had we not found spread into the peritoneal cavity. The pathologist called into the operating room and confirmed the presence of metastatic cancer in all of the peritoneal biopsy specimens. We closed the fascia and then the skin. The anesthesia and operating room staff were eerily silent as I pulled off my gown and gloves and began the long walk.
Informing the relatives
I first traipsed back to the pathology suite to look at the slides for myself. I took the Baylor College of Medicine third year medical student with me as we then trudged to the surgical waiting area. I walked into the consultation room with the medical student and we faced the upturned, concerned gazes from the patient's family seated in the small room. They knew from the warning conversation yesterday and from the look on my face the news was not good. I quietly and thoroughly explained what I found on my examination of the peritoneal cavity and the findings of the intra-operative ultrasound. The family, in the stunned and disbelieving early phase following delivery of such information, initially asked a few questions about next steps. I reported this was not a problem I could fix with an operation, and systemic chemotherapy delivered through an intravenous port would be the next treatment to consider. Predictably, I was asked about the success rate of such therapy and I dutifully and painfully informed them chemotherapy would possibly prolong his life by several months, but would have essentially no likelihood of curing him of this advanced stage IV cancer. I added the chemotherapy could be associated with significant side effects and toxicities affecting his quality of life. I delivered a hard, truthful, and delicate discourse on the truly unfortunate situation caused by this man's cancer.
Coping with the bad news
Disbelief and shock turned into tears. The third year medical student, who had asked me if he could accompany me to see how I delivered this difficult and heart-breaking news, quietly slipped out of the door and returned with a box of tissues. I noted with gratification he went from family member to family member and offered them a tissue and a comforting touch of his hand on their shoulders. We academic medical school faculty sometimes worry about the millennial generation being different, and possibly even indifferent. This young man offered me reassurance there is compassion, feeling, and care among our current generation of trainees and there is great hope for the future of medicine as a profession that attracts those who want to provide care and assistance for those in need.
I spent about 15 minutes in the room with the family and answered all questions. I reassured them several times I would be available later in the day and at any time in the future to provide assistance and further information. The family asked me if they could be present when I reported the findings to the patient, and I replied I would bring some of them with me after he was awake and alert enough from anesthesia to understand a conversation.
About an hour after taking the long walk, and after I had spent 10 minutes in quiet reflection sitting alone in a chair in the surgeons' locker room to gather my own thoughts and sort my own emotions, I went with one of the recovery room nurses and fetched three members of the family. We walked to the patient’s bedside in the recovery room where I repeated the explanation of the intra-operative findings to the patient. He was calm but appropriately disappointed. He asked several of the same questions the family had asked, and I reported we would obtain detailed pathologic and genetic studies from the tumor biopsies I performed to guide treatment decisions. At the end of our conversation, he took his right hand from under the blanket and stoically shook my hand saying, “Thank you for doing your best, Doctor.”
Providing medical and emotional support
I have taken the long walk numerous times every year for over 30 years now. Some weeks or months it seems there are more of the long walks, but I realize it is random probability and chance because at times we win more battles with cancer than at other times. It has not become any easier, and the walk does not seem any shorter. The feelings of sadness are no less raw. I am still amazed and impressed by the dignity, grace, and consideration demonstrated by patients and their family members after I deliver bad news and they recover from the initial overwhelming fear and grief. I know I will have colleagues who disagree, but I believe it is important to continue to feel and demonstrate genuine emotion and authentic concern. All of us dedicated to a career in medicine providing care for our fellow human beings must make the long walk on occasion. For those of us in oncology, the frequency may be greater, but it doesn’t mean we are any better at delivering tough information with heartfelt and thoughtful compassion.
In surgery, we may need to make the long walk when, like today, the cancer is unexpectedly widespread and not amenable to the planned surgical procedure. Other times, a complication or problem may occur during an operation for benign or malignant disease and we must dutifully, honestly, and transparently reveal and discuss the event and the implications. Not an easy task because surgeons never want a patient to suffer an unfortunate event or outcome during an operation, and the feelings we have of guilt, remorse, and self-doubt must be subdued temporarily to provide a thorough description and disclosure to the family and patient. In our hospital, the long walk is not very far if one actually measures the distance traversed, but it feels longer over the years as I steel myself for the onslaught of emotion I will face from distraught family and friends. They have the right, perhaps even the cleansing need, to express a full range of vigorous emotion, and our job as physicians and surgeons is to listen and to provide comfort, information, and support.
Final thoughts: Crucial physician-patient-relationship
In this era of rapid accumulation of data and technology impossible to digest and know completely, I feel an imperative to emphasize, teach, and model kindness, concern, and compassion for our patients and our colleagues in all disciplines. As patients, most of us have encountered the occasional physician who doesn’t make any more than cursory physical contact with us and whose eyes are glued to a computer screen while he or she mechanically asks questions typing responses and information into an electronic medical record. Such depersonalization leads to dissatisfaction and disruption of the crucial physician-patient relationship.
We should not forget or forego our humanity despite the pressures of too much information, too much time spent with the mandatory electronic medical record, and too much energy wasted with piles of paperwork, meetings, and insurance verification. If we accept mediocrity in the care we provide, we will have a 100% success rate. If we are willing to push the envelope, if we expect excellent, exceptional, and extraordinary effort at all times, we will have disappointments and failures, but we will also achieve spectacular successes.
I believe as we continue to learn more about preventing and effectively treating cancer, the long walks will become less frequent. Hopefully that will happen sooner rather than later, but cancer is an insidious opponent. We must fight on with our research and clinical colleagues to discover novel treatments and techniques to improve the lives and outcomes of our patients.
And we should provide hope and continued care tempered with earnest, honest, and realistic information and expectations every time we make the long walk.