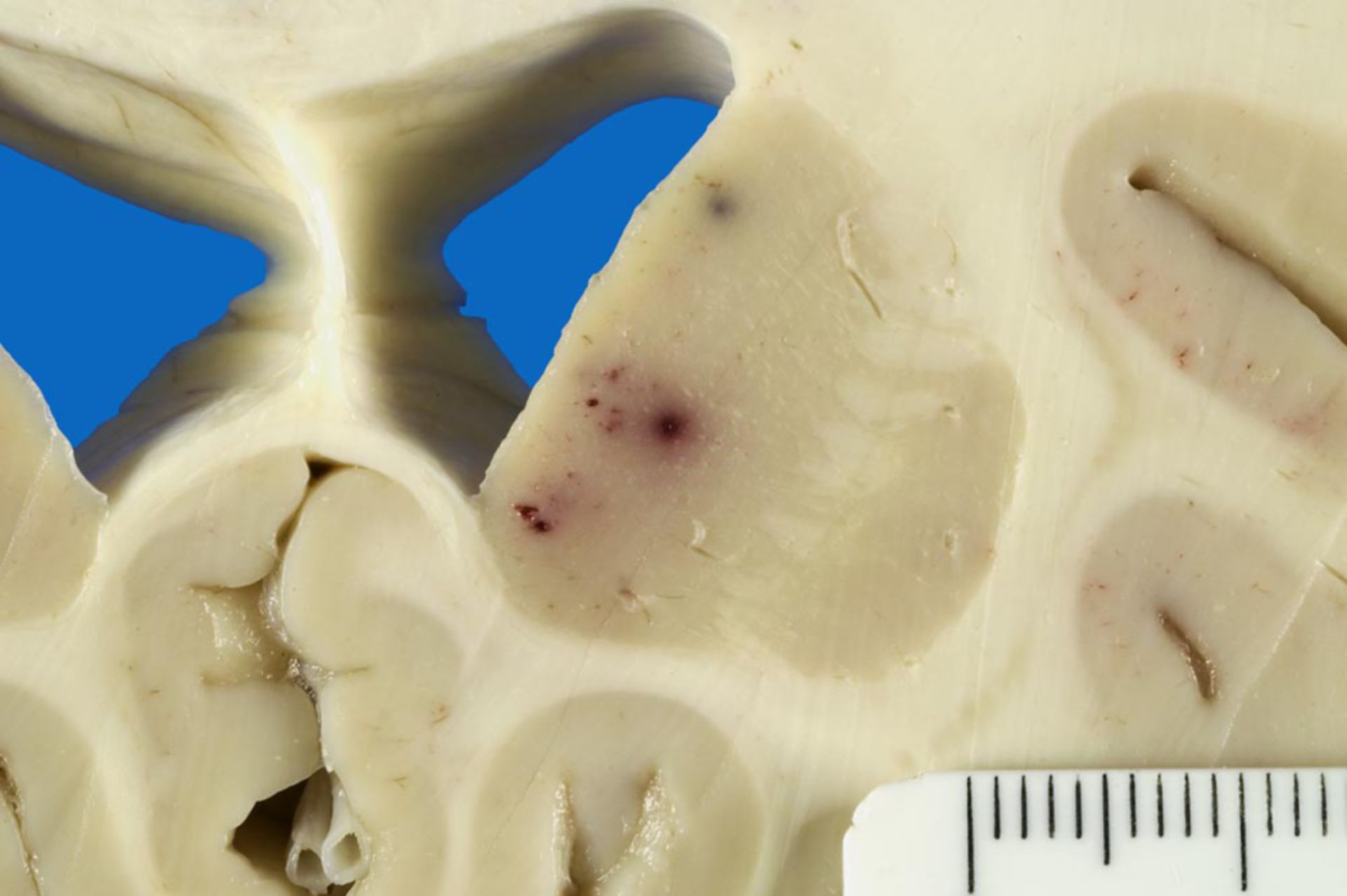
Diagnosis: Petechial hemorrhages in the Thalamus in an infection with HHV-6 (human herpes virus 6)
Description: The picture shows fresh petechial hemorrhages in the Thalamus.
Additional finding: In the course of the neuropathological dissection of the brain, macroscopic smaller, fresh petechial hemorrhages were found in the Striatum, Thalamus, Amygdala, and Hippocampus. The micropscopic preparation of specimen taken from these regions has confirmed the macroscopic picture, yet moreover, it has shown an extensive bilateral sclerosis of the Hippocampi. There was a subtotal nerv cell loss in the area of the hilus and the CA3-region, moderate neuronal deficits in the CA2-sector, and an almost complete nerve cell death in the area of Sommer's sector. Another noticeable thing was an extraordinarily strong reactive astrogliosis within the whole hippocampal region and within the Amygdala.
Clinical history: 29 year old male patient, acute lymphatic leukemia (ALL) known for 3 years. Allogenic stemm cell transplant 9 weeks before death.
Comment: This unusual macroscopic and microscopic findings are consistent with a clinically suspected HHV-6 reactivation in a condition after a hematopoiectic stemm cell transplantation. The occurence of fatal HHV-6-associated encephalitis after bone marrow transplants is described in literature for a long time (see Drobyski WR et al., NEJM, 1994), likewise, there are reports concerning hippocampal sclerosis in the course of a HHV-6-associated limbic encephaltis (in condition after stem cell transplantation; Wainwright MS et al., Ann Neurol, 2001). The occurence of petechial hemorrhage in the CNS-tissue can rather be interpreted as happening in the course of a thrombotic micoangiopathy and can equally be found in literature in association with a HHV-6 encephalitis after stemm cell transplantation ( Belford A et al., Am J Hematol, 2004). After all, also the extensive astrogliosis of the amygdala/ between the hippocampi observed in the present case, can be traced back to a recently reportes tropism of HHV-6 for hippocampal astrocytes (see Fotheringham J et al., J Infect Dis, 2007). In summary, due to the clinical progression and the macroscopic and microscopic findings of the neurpahological dissection, one can securely assume the presence of a HHV-6 associated hippocampal sclerosis with concomitant, also HHV-6-associated hemorrhages on the base of a thrombotic microangiopathy, even if the PCR-based viral proof are not to be counted as evidence because of the 90% seropositivity.
(Source: ©PathoPic)